%20(1).png)

The Safe Pain Protocols: How to Know When to Push Through and When to Back Off
You’ve been told, “If it hurts, stop doing it.”
Rest. Protect yourself. Don't do anything that makes it worse.
I get it — when you're dealing with back pain or sciatica, the fear of making things worse is very real. Some of you have had terrifying trips to the emergency room or been bedridden for weeks at a time from a flare up.
OF COURSE YOU WANT TO AVOID FLARE-UPS.
But here’s the thing… If you baby yourself, that’s going to make things worse as well.
We need to find a balance between “too much too fast” and “too little for too long.”

The truth is there's a difference between SAFE pain and UNSAFE pain. Knowing the difference (and actually being able to apply it in real life) is one of the most powerful skills you can develop on your road to recovery.
In fact, this is the topic we spend MORE coaching time on than almost anything else with our clients inside the Beyond Back Pain program. Because it sounds simple in theory, but in practice? It's where everyone gets confused — and where we get the most questions in the chat.
- “Hey I think I’m getting some tingling in the glute during ____ exercise… Is that centralization?” (Answer: probably not)
- This week I’ve noticed more tightness in the hip and groin and I’m not sure if that’s a “No Worse” issue and I should back off exercises?” (Answer: We gather more information about “what’s in the cup?” to see if there are non-physical factors like stress, sleep, and life situations that are impacting pain, and we may or may not need to change exercises, and/or focus on lifestyle changes)
You get the idea. It’s hard to apply this stuff when you’re in pain.
So in this article, I'm going to break down our Safe Pain Protocols in full — what they are, what the research says about exercising with pain, how all three principles work TOGETHER, and how we apply them with clients when things get tricky.
Just please understand that there’s a HUGE difference between reading something, and applying it in real life.

It takes some trial and error and that’s normal. It’s okay to have ups and downs, but over time as you learn how your body responds and feed your brain evidence of safety, you’ll start to feel like you’re in control.
In this article we'll cover:
- Hurt does not equal harm: What the research actually says
- Why imaging findings like disc herniations are misleading
- What the Safe Pain Protocols are (as a complete system)
- The Pain Traffic Light: Your guide during activity
- The No Worse Principle: Your guide after activity
- The Centralization Principle: Your guide for nerve symptoms
- How all three work TOGETHER, not in isolation
- The Rule of Too's — the trap on both sides
- Why this is so hard to do alone — and real client stories
- How we apply this inside Beyond Back Pain
- Where to go from here
Hurt Does Not Equal Harm
Let me say it clearly: just because something causes pain doesn't mean it's dangerous.
This is one of the most important things you can understand about chronic pain — and it's one of the most misunderstood.
Here's why it matters. People with chronic back pain often develop what researchers call kinesiophobia.
Kinesiophobia — Excessive fear of movement, often arising the belief that movement will cause further damage. This often results in overprotective/avoidant behavior.
Studies show these fear-avoidance beliefs are actually among the strongest predictors of long-term disability and inability to return to work - not the imaging findings on your MRI, not the severity of your herniation, not your posture. Fear of pain can become MORE disabling than the pain itself. [1]
And here's where it gets really interesting.
A systematic review and meta-analysis directly compared people who exercised INTO mild-to-moderate pain versus people who only did completely pain-free exercise. The group that exercised with some pain actually had BETTER immediate outcomes. [2] The researchers concluded that pain during therapeutic exercise for chronic musculoskeletal conditions doesn't have to be a barrier to successful outcomes.
Let me say that again: exercising into some pain produced slightly BETTER results than avoiding pain entirely. [2]

At the very least, it’s perfectly safe to have some pain during exercises. Even today I get sore after deep mobility-based deadlift/good-morning variations as pictured above, but now I think of it like normal post-exercise soreness. It goes away, and I get stronger.
So if you're babying yourself - avoiding every twinge, canceling every exercise session at the first sign of discomfort - you're not protecting yourself. You're keeping yourself stuck. You're never going to get stronger. You're never going to get better. You're going to live in a life of fear and avoidance that makes everything worse. [Insert soapbox rant 😅]
Quick note #1: I want to be crystal clear. This does NOT mean "no pain no gain" and it does NOT mean push through everything regardless of severity. That approach will absolutely flare you up. This is about learning the DIFFERENCE between safe and unsafe pain — which is exactly what the Safe Pain Protocols are for.
Why MRI & X-ray Imaging Findings Are Misleading
Before we get into the protocols themselves, we need to address something that keeps a LOT of people stuck: their MRI results.
You've been told your pain is coming from your alignment. Your disc herniation. Your short leg. Your pelvic tilt. Your nerve compression. I understand why that sounds scary. But in most cases, as long as there are no red flag symptoms, the MRI findings just don’t matter very much.
Brinjikji and colleagues did a huge (and rather famous at this point) study on asymptomatic (PAIN-FREE) people. [3]
You’d expect that pain free people would have really healthy looking spines on their MRI, right?
Wrong. Here are some stats… [3]
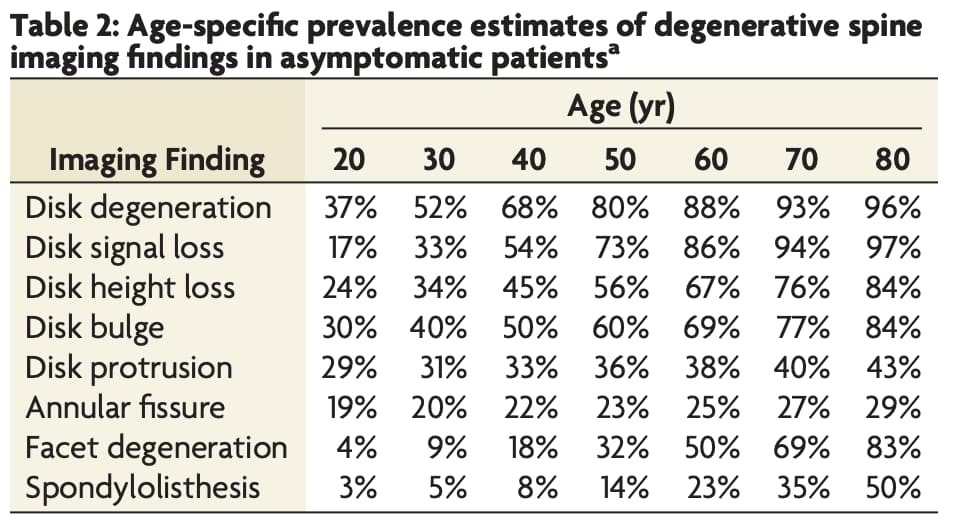
By age 50, 80% of SYMPTOM-FREE PEOPLE will have degeneration, 60% have a disc bulge, 36% have a disc protrusion, 23% have an annular fissure, and 14% have a spondylolisthesis. See the table above for all age ranges and conditions in this study.
As long as your doctor has ruled out red flags, stop worrying about your MRI.
Saem goes for asymmetries and imbalances. Everybody has asymmetries. For example most people have an anterior pelvic tilt (75-85% of asymptomatic people), that’s just normal skeletal formation for most people. [12]
Psst — this is also why we don't let imaging results dictate your exercise program. Two people with the exact same MRI might respond completely differently to the same exercise.
We care about how your body RESPONDS to movement. And that's exactly what the Safe Pain Protocols help you assess.
The Safe Pain Protocols — An Overview
Credit where credit is due: We didn’t invent this. Some elements of this are commonly used by the McKenzie Method, Annie O’Connor, and others. We just combined it in a way that makes sense from our experience.
We call these three principles together our Safe Pain Protocols.
They apply to everything — not just your formal exercises in the program. Mowing the lawn. Doing chores. Cleaning the house. Going for a walk. Going on a trip. Any activity in your life, for the rest of your life. And honestly? They apply to most types of muscle, joint, and nerve pain — not just back pain and sciatica.
The three Safe Pain Protocols are:
- The Pain Traffic Light - your guide DURING activity
- The No Worse Principle - your guide AFTER activity
- The Centralization Principle - your guide for radiating symptoms
FYI - you need to use ALL of these together (plus the “what’s in your cup?” concept) to answer the question “is this exercise appropriate for me right now?”

Protocol #1: The Pain Traffic Light (Symptom Traffic Light)
The Pain Traffic Light is your guide DURING exercise and activity. And yes — I call it the "pain" traffic light, but it really applies to ALL symptoms: pain, numbness, tingling, heaviness, burning, electrical sensations, weakness. Any sensation you're tracking.
Here's how the scale works:
- Green Light (Mild — 1 to 3/10): Green Means Go. Keep going. This level is fine. A lot of people wouldn't even call this "pain" — they'd describe it as uncomfortable, achy, or just a sensation. Green means go.
- Yellow Light (Moderate — 4 to 6/10): Yellow Means Slow down. You can probably keep going, but ease off a bit. Pay attention. Yellow means proceed with caution.
- Red Light (Severe — 7 to 10/10): Red Means Stop. Do something else instead. This level of symptom during activity is too much. Red means stop.
“But I hate rating my pain from 1-10!”
Yea I know. But it works. All that matters is that whatever YOU call a 6 remains consistent over time, so YOU can judge what’s “too much.”
For additional context:
- Zero out of ten is completely normal, zero symptoms.
- Ten out of ten is "I need to go to the hospital right now."
Quick note: The traffic light only tells you what's happening IN THE MOMENT. It says nothing about whether an exercise is appropriate for your program long-term. That's what the next principle is for.
Protocol #2: The No-Worse Principle
The No Worse Principle asks: how do you feel AFTER activity? Not just in the moment — but later that evening, the next day, days after, or even across weeks and months of consistent exercise?
Here's the question you're always asking: Are my symptoms getting worse? Better? Staying the same?
Some muscle soreness after exercise is completely normal. That's EXPECTED. What's unhelpful is if your baseline symptoms are trending upward over time - if things you used to do without pain (like putting on your shoes, walking to the mailbox, sitting through dinner) are now causing more pain than before you started. That's a signal. Something's too much and we need to ease off.
Here's the critical thing that most people miss: this isn't just about the next morning. The No Worse Principle applies across MULTIPLE time horizons:
- During activity (overlaps with the Traffic Light)
- That evening after activity
- The next day
- Several days after a session (delayed onset pain is very common)
- Across weeks of a consistent program
- Across months - where gradual overtraining can quietly creep in
Listen up!
We see clients who are doing great week-to-week, but over two or three months of gradually increasing their activity, their symptoms start gradually getting worse. That's overtraining territory. If you're consistently doing more and your symptoms are consistently getting worse — not just temporarily after a hard session, but trending in the wrong direction overall — we need to look at your load and make adjustments.
Or even if your symptoms are fine but you’re hitting a plateau with your exercise progressions, you might want to watch for other signs of overtraining and potentially take an easy week to reset.
The No Worse Principle doesn't have a single cutoff. It requires you to zoom out and look at your TRAJECTORY, not just today's session.
Protocol #3: The Centralization Principle
This one is specifically for people with radiating symptoms — sciatica, nerve pain, leg pain, foot numbness, calf tingling, weakness, heaviness, or similar traveling sensations.
Note: Weakness in the foot/toes should always be evaluated first by a doctor to rule out nerve damage.
The concept comes from the McKenzie Method, and it refers to the direction that pain MOVES. [4] Here's the core idea:
- Pain traveling MORE distally (further down the leg, into the foot or toes) = bad. This is called peripheralization or radiation, and it suggests you're irritating the nerve. Stop what you're doing, ease off, try something different.
- Pain pulling UP toward the spine (less leg pain, less foot numbness, even if your back feels a little more sore) = good. This is centralization, and it's a reliable marker of a favorable outcome. [5]
Research has confirmed this repeatedly. One study found that patients who demonstrated centralization had significantly better functional outcomes, fewer treatment visits, and higher rates of returning to work compared to those whose symptoms didn't centralize. The study found that non-centralization and leg pain at intake were the strongest predictors of developing chronic pain and disability — not the structural findings on their MRI. [4]
Another study found that in a review of 87 patients with radiating leg pain, centralization occurred in 76 of them — and its presence during initial evaluation was described as a very accurate predictor of successful treatment outcome. [6]
It’s a simple concept. If moving in one direction feels good and the other direction feels bad, ease off a little on the sensitive movements and lean into the good movements.
Quick note: Some of you have a really specific symptom pattern — a lot of pain in the glute or hip, then nothing in the middle of the leg, but then foot numbness or calf tingling. Treat those distal (far) symptoms the same way. Ease off things that irritate the foot or calf symptoms and gradually reintroduce as symptoms allow. Favor activities that settle the foot/calf symptoms down.
How All Three Work Together
These three protocols don't work in isolation. You have to evaluate ALL of them together. Think of it like a checklist: an activity only gets a green light if it passes ALL THREE tests. If it violates any one of them, you need to modify, regress, or skip.
The good news is that if it passes all of these criteria, AND you’ve done the same level of exercise enough times over days or weeks to know it’s not going to flare you up… CONGRATS! It’s time to progress to harder exercises! Yipee!
Let me give you some examples of how they interact:
Scenario 1: You do an exercise and your symptoms centralize (good!) — but the pain was a 7/10 during the exercise (red light). That's a bit too much. The centralization is encouraging, but the intensity is too high. We need to find a way to get the same centralization benefit at a lower symptom level — maybe through a modified version, reduced range of motion, or a different position.
Scenario 2: You do an exercise at a 3/10 (green light) and it centralizes (good!) — but the next morning, your baseline symptoms are noticeably worse and even putting on your socks (which was fine the day before) is now very challenging. That's a violation of the No Worse Principle. Even though it seemed fine in the moment, your body's telling you the overall load was too much.
Scenario 3: You do an exercise at a 5/10 (yellow light), symptoms don't worsen overnight, and nothing peripheralizes. That's actually a pass on all three — proceed but definitely don’t increase intensity yet, but you can probably keep going. Monitor over days/weeks to re-evaluate.
Scenario 4: Symptoms centralize, traffic light is green, no worse overnight — but after 6 weeks of consistent training, your baseline pain has slowly crept upward. That's a No Worse violation on the long timeline. Time to back the volume off and see if things settle. Unless of course you find that over the last 6 weeks some outside life factor has been “off” so to speak - like stress, sleep, nutrition, etc… In which case keep exercising but manage the life factors that are leading to your system being overwhelmed.
This is why we say: if it violates ANY of the three protocols, it's generally a sign to ease off. You modify, skip for that day, or choose an alternative.
The Rule of Too's
If you do too much for too long, you get injured.
If you do too little for too long, you never progress, you become weak, and you’re more easily injured due to weakness.
Or, a lot of people do too much too fast after a long period of too little for too long, and flare things up.
Too much too fast leads to injury and flare-ups. You push through red light pain, ignore the “No Worse” signals, keep doing exercises that peripheralize your symptoms — and you end up worse than when you started. This is the overzealous approach that sets people back weeks.
The most common way this happens is that people get excited when they start exercising again, and since it feels fine in the moment, they push like they used to… And the next day they can barely get out of bed due to horrible pain.
Don’t skip steps!
Too little for too long leads to weakness, deconditioning, and chronicity. You avoid ALL sensation, avoid every exercise the moment any symptoms show up, stop moving the moment you feel any discomfort - and you never get stronger. Your nervous system learns that movement equals threat. Your body deconditions. You stay stuck in a painful, fearful cycle that gets harder and harder to escape. [7]
Don’t baby yourself either!
The Safe Pain Protocols exist in the space BETWEEN those two extremes.
Be like Goldilocks - not too much, not too little.
It’s not about being fearless or wreckless.
It’s not about white-knuckling through everything and pushing through pain.
It’s about being SMART, systematic, and patient - building your capacity to tolerate more over time, with clear guardrails to protect you along the way.
And here's what the research tells us: exercise is one of the most effective treatments on the planet for chronic low back pain…
A major Cochrane review of 249 randomized controlled trials found that exercise therapy is more effective than no treatment, usual care, or placebo for both pain and disability — both short term and long term. [8] Exercise (as well as education, and cognitive behavioral therapy) is also recommended as the FIRST line of care for chronic low back pain by current clinical practice guidelines. [9]
Motion is lotion. The question is just HOW to move intelligently.
- How much?
- How often?
- How intense?
- When to progress/regress/modify?
If that seems like a lot to figure out on your own, we’re happy to write you a step-by-step plan and have real human beings (who happen to be experts) guide you to feeling better, stronger, and more in control. Just join the FREE GROUP to learn more about working with us 1-on-1.
Why This Is So Hard to Do Alone
From personal experience and from working with over 1,000 people with chronic pain, I know that these three protocols are simple to understand in concept. But in practice they're frustrating to apply without reassurance.
And I say that not to discourage you — but because I've watched it play out with so many clients.
People read about the traffic light, nod along, then message me three days into their program: "I had some tingling during the deadbug — does that count as yellow? I also felt it a little the next day but it went away by afternoon. And sometimes my foot goes numb for no reason. Am I okay? Should I skip? Should I push?"
That's not a lack of effort. It’s not even a lack of knowledge. It’s a lack of repetitions in THEIR body, and a lack of real-world feedback and confidence.
That's a genuinely hard clinical judgment call - especially when you're scared, when any sensation in your body feels like a potential disaster, and when you've been told for years that your back is fragile and broken.
One of the most common patterns we see in new clients is that they interpret EVERY sensation - including totally normal post-exercise muscle soreness - as a danger signal.
They assume any discomfort means they're re-injuring themselves. They stop before they should. They don't build any strength or tolerance. They get discouraged because they're not making progress. This is the fear-avoidance cycle — and it's been shown to be one of the biggest drivers of long-term disability in back pain. [10]
On the flip side, we also see the opposite - clients who are used to pushing through everything, who have a "no pain no gain" history, and who don't know how to recognize when they've genuinely crossed a line.
They flare up, rest for a week, try again, flare up again. The on/off, weekend-warrior cycle is exhausting and demoralizing.
Both of these patterns are why having experienced coaches walking you through this - responding to your specific symptoms, adjusting your specific exercises, telling you "that's normal muscle soreness, keep going" or "that tingling is worth addressing, let's modify" - makes an enormous difference.
Research shows that individualized exercise programs, especially when combined with education that addresses fear-avoidance beliefs, produce significantly better outcomes than generic programs. [11]
I know a lot of you are trying Do-It-Yourself programs that only offer a cookie-cutter exercise approach, without 1-on-1 support, and without the ability to personalize your plan based on your abilities, limitations, history, and goals.
That’s only going to get you so far. It’s the same problem with in/out 5min doctor’s appointments. Without getting to know YOU, how can they help? Without teaching you how to make decisions based on YOUR body, how are you going to work around your roadblocks?
So if you're stuck right now — reach out to learn about our Beyond Back Pain Program. This is exactly what we're here for.
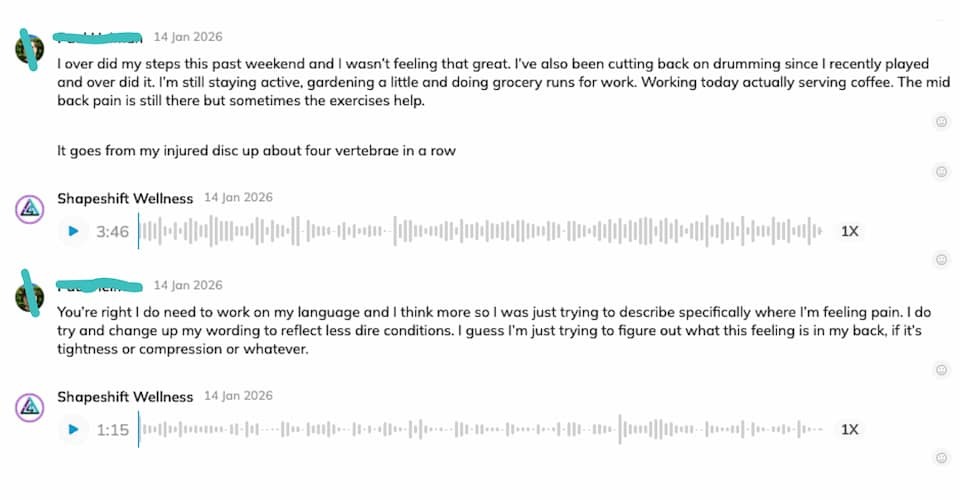
Real Client Stories: What This Looks Like in Practice
Let me share what a couple of our clients experienced — because this is so much clearer in a real example than in theory.
One of our clients, Hannah (name changed for privacy), came to us with a full list of findings on her MRI: L4-L5 slipped disc, sciatica, degenerative stenosis, pinched nerve, and scoliosis she'd had since 17.
When we met, her pain had become so debilitating she had to go straight from work to an ice pack every night. She couldn't walk more than a block without needing to sit down. She'd been through two traumatologists, four physiotherapists, acupuncture, and massage. Classic “I’ve tried everything.” What she described as the pivotal difference with our program was the graded exposure approach, and the ability to communicate in real time: "that exercise didn't feel right - can we change it?" And hearing back immediately: yes, try this instead.
She put it perfectly: "I became fearful of my body. I was scared to move. I didn't know what was good, what was bad." That's the fear-avoidance pattern in a nutshell. And now? She's hiking in the mountains. She's traveling. She's playing music again. She went from being unable to walk a block to spending full days on her feet with her friends. Same spine. Same MRI findings. Completely different life — because she learned how to move SAFELY, not fearfully.
Another client described exactly the boom-bust cycle that the Rule of Too's is designed to prevent.
She'd do things that felt okay in the moment, have a flare-up, rest for three days, try again, have a worse flare-up, tell herself she needed to rest for a whole month. She was swinging between too much and too little with nothing in between. The shift happened when she started using the Safe Pain Protocols as her actual guide. That, combined with having someone in her corner saying "Walk three minutes, not sixteen. Lean into ___ exercise. Skip _____ for now." The frequency, intensity, and duration of her flares all decreased consistently from that point forward. Within months, she was taking cross-country trips and running between airport terminals without a single flare.
"The problem wasn't so much that the pain hurt," she said. "It was the fear I had and the way it was stopping me from living my life."
When she understood that a flare wasn't re-injury — it was just her sensitive nervous system reacting — everything changed. Sensitive does NOT mean dangerous.
How We Apply This Inside The Beyond Back Pain Program
Inside the Beyond Back Pain program, the Safe Pain Protocols aren't just a concept we explain once and move on from. They're the backbone of how we coach every single exercise decision, every single day.
Here's what that looks like in practice:
Exercise progressions, regressions, and modifications.
Every exercise in your program has easier versions, harder versions, and alternatives. When you apply the Safe Pain Protocols and something doesn't pass the test, we don't just tell you to skip it and do nothing. We find the version that works for you RIGHT NOW. The goal is always to find the most challenging exercise you can still do within green-yellow symptom territory, without worsening over time, and without peripheralizing your symptoms. That version is your entry point — and we build from there.
Real-time coaching in the app.
When clients message us in the chat saying "I had tingling during X, what should I do?" — that's a Safe Pain Protocol conversation. We're not guessing. We're teaching you how to ask yourself: what color light? What was it during and after? Did anything travel further? What's my baseline been like this week? From those answers, we can help you decide whether to keep going, modify, or skip. That's the protocol in action — applied to YOUR specific body, YOUR specific symptoms, YOUR specific exercises.
Group coaching calls.
We regularly walk through specific examples of how these principles apply to real exercises and real daily activities — because the nuances are endless. Does bending forward count if it only hurts at the very end of range? What if the pain goes away after the first few reps? What if I feel it the next morning but it's totally gone by noon? These are the questions that come up constantly, and working through them live, with me (Dr. Davis) and Dr. Blake beats trying to figure it out alone every time.
Calm shit down, then build shit back up.

If you're in a flare and you're consistently violating the No Worse principle, if your symptoms are peripheralizing, if things are clearly trending in the wrong direction, we pump the brakes. We calm shit down, then build shit back up. That means temporarily reducing load, volume, or intensity until your nervous system settles, then resuming with a more gradual progression. This isn't failure. It's intelligent pacing. And it's a core part of how we use the protocols to manage overtraining before it becomes a serious setback.
This is one of the biggest issues people have: If something doesn’t go according to plan, they completely stop what they were doing and bounce to “the next thing.” But we PLAN for things to not go according to plan. Having a backup plan IS PART OF THE PLAN. Remaining consistent when you get knocked off track is the most important part of the process. Otherwise every bump just resets the clock.
The whole system — the Traffic Light, the No Worse Principle, the Centralization Principle — it's designed to give you the CONFIDENCE to move. Not just the permission. The confidence. Because confidence backed by a clear framework is what actually changes behavior for the long haul.
The Bottom Line
If you've been sitting on the sidelines because you're afraid that any pain means damage — hear this clearly: you're not protecting yourself. The research is unambiguous that exercise, even with some discomfort in the process, leads to better outcomes for people with chronic back pain and sciatica. [2] Avoidance, on the other hand, leads to more fear, more deconditioning, and more disability. [1]
But if you've been pushing through everything without a framework — and you keep flaring up — the Safe Pain Protocols are your roadmap. They tell you exactly when to push, when to ease off, and when to stop.
- Green means go. Yellow means slow down. Red means stop.
- No worse - if symptoms are trending upward over days, weeks, or months, dial back the load.
- Centralize - favor movements that bring symptoms toward the spine, avoid movements that drive them further down the leg.
Simple. Clear. Evidence-based.
And absolutely non-trivial to apply in real life without guidance.
If you're ready to start applying this with actual coaching support - with a personalized exercise program, real-time feedback on your symptoms, and a team that's walked hundreds of people through exactly this process - come check out the Beyond Back Pain Program. This is what we do, every day, for people exactly like you.
And if you're not ready to jump in yet — bookmark this article or Join the FREE group for free trainings and resources.
References
- Wertli MM, Rasmussen-Barr E, Weiser S, Bachmann LM, Brunner F. The role of fear avoidance beliefs as a prognostic factor for outcome in patients with nonspecific low back pain: a systematic review. Spine J. 2014;14(5):816-836.e4. doi:10.1016/j.spinee.2013.09.036. PMID: 24412032. View on PubMed
- Smith BE, Hendrick P, Smith TO, et al. Should exercises be painful in the management of chronic musculoskeletal pain? A systematic review and meta-analysis. Br J Sports Med. 2017;51(23):1679-1687. doi:10.1136/bjsports-2016-097383. PMID: 28596288. View on PubMed
- Brinjikji W, Luetmer PH, Comstock B, et al. Systematic literature review of imaging features of spinal degeneration in asymptomatic populations. AJNR Am J Neuroradiol. 2015;36(4):811-816. doi:10.3174/ajnr.A4173. PMID: 25584808. View on PubMed
- Werneke M, Hart DL. Centralization phenomenon as a prognostic factor for chronic low back pain and disability. Spine (Phila Pa 1976). 2001;26(7):758-764. doi:10.1097/00007632-200104010-00005. PMID: 11295896. View on PubMed
- Sufka A, Hauger B, Trenary M, et al. Centralization of low back pain and perceived functional outcome. J Orthop Sports Phys Ther. 1998;27(3):205-212. doi:10.2519/jospt.1998.27.3.205. PMID: 9513866. View on PubMed
- Donelson R, Silva G, Murphy K. Centralization phenomenon: its usefulness in evaluating and treating referred pain. Spine (Phila Pa 1976). 1990;15(3):211-213. doi:10.1097/00007632-199003000-00012. PMID: 2141186. View on PubMed
- Booth J, Moseley GL, Schiltenwolf M, Cashin A, Davies M, Hübscher M. Exercise for chronic musculoskeletal pain: a biopsychosocial approach. Musculoskeletal Care. 2017;15(4):413-421. doi:10.1002/msc.1191. PMID: 28371175. View on PubMed
- Hayden JA, Ellis J, Ogilvie R, Malmivaara A, van Tulder MW. Exercise therapy for chronic low back pain. Cochrane Database Syst Rev. 2021;9(9):CD009790. doi:10.1002/14651858.CD009790.pub2. PMID: 34580864. View on PubMed
- Foster NE, Anema JR, Cherkin D, et al. Prevention and treatment of low back pain: evidence, challenges, and promising directions. Lancet. 2018;391(10137):2368-2383. doi:10.1016/S0140-6736(18)30489-6 View on PubMed
- Zale EL, Lange KL, Fields SA, Ditre JW. The relation between pain-related fear and disability: a meta-analysis. J Pain. 2013;14(10):1019-1030. doi:10.1016/j.jpain.2013.05.005. PMID: 23850095. View on PubMed
- Fleckenstein J, Floessel P, Engel T, et al. Individualized exercise in chronic non-specific low back pain: a systematic review with meta-analysis on the effects of exercise alone or in combination with psychological interventions on pain and disability. J Pain. 2022;23(11):1856-1873. doi:10.1016/j.jpain.2022.07.005. PMID: 35914641. View on PubMed
- Herrington L. Assessment of the degree of pelvic tilt within a normal asymptomatic population. Man Ther. 2011;16(6):646-648. doi:10.1016/j.math.2011.04.006 View on PubMed
.jpg)



